Looking for information about other Dental Topics?
Full Website Index• Animated-Teeth.com •

Guide to dental white-spot lesions – Causes, Prevention, and Treatment.
Guide to dental white-spot lesions.
White-spot lesions are the earliest visible sign of tooth decay. And, as good news, if they’re detected soon enough, just improving your daily oral care routine may be all it takes to keep them from progressing into a full-fledged cavity.
This guide covers everything you need to know about these lesions—from what causes them and how to prevent them, to the treatment options available when repair is necessary. (Check out this page’s Table of Contents for a complete list of its topics.)
By understanding the early warning signs, you can take action before significant tooth damage has occured.
1) What are white-spot lesions?
White spot lesions form on a tooth’s enamel (especially in areas near the gum line or next to bonded orthodontic brackets) and are an early indication of tooth decay formation. In fact, a white spot is the first readily visible sign that a cavity is beginning to develop. Another term dentists use for white spots is “incipient lesions.”
a) What do the lesions look like?
True to their name, affected enamel surfaces have an opaque, chalky white appearance that is lighter in color than the surrounding undamaged areas. These white patches can range from barely visible to quite noticeable, depending on their degree of development.
b) Where do they form?
Since they are caused by the same process that leads to tooth decay, white spot lesions are typically found in areas where oral hygiene has been poor and dental plaque has been allowed to accumulate and persist.
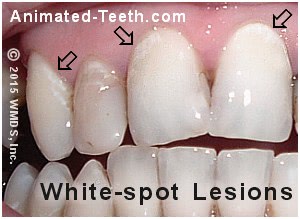
White spot lesions are frequently found near the gum line (areas that have been difficult to keep plaque-free).
Likely locations:
- It’s very common to see these white patches form right at a tooth’s gum line—an area people frequently miss when brushing. (See picture above.)
- In similar fashion, if you’re not flossing well enough (either not as often as you should or you aren’t doing it effectively) you may discover that white spot lesions have formed in the areas where your teeth touch together.
- And since cleaning around dental braces can be difficult, it’s common to see these lesions form adjacent to bonded orthodontic brackets (see picture below). (We discuss the increased risk of white spot lesions with orthodontic patients here.)
So anywhere you notice a buildup of white material on your teeth—meaning dental plaque and related debris—like along the gumline or around orthodontic brackets, the tooth enamel underneath is at risk of developing a white spot lesion.
c) What causes white spot lesions to form?
They’re caused by enamel demineralization (decalcification), which is the process that causes tooth decay and ultimately cavities. It occurs when a tooth’s surface is exposed to acidic waste products produced by oral bacteria living in dental plaque.
How does enamel decalcification result in white spots?
As the demineralization process takes place, the affected area begins to lose some of its mineral content. This includes both hydroxyapatite crystals (enamel’s dominant building block), as well as calcium, phosphate, and other ions.
- Initially, the greatest amount of damage takes place at a level just below the tooth’s surface (10 to 15 microns, which is about 1/10th the width of a human hair).
The explanation for this lies in the fact that the surface enamel of teeth is typically far more resistant to the demineralization process than that which lies deeper, and thus remains less affected. (The enamel’s history of exposure to fluoride can play a big role in creating this “harder” surface effect.)
- As the surface and subsurface changes progress, they affect the optical (light-handling) properties of the enamel. As a result, the surface of the affected area starts to lose its shine and glossiness, and overall the lesion begins to take on a lighter, chalky-white appearance. (Hence the name white spot lesion.)
- As the demineralization process progresses underneath, the tooth’s surface becomes an impromptu “lid” over the lesion (2 to 50 microns in thickness). As more and more mineral content is lost from it, its original intact surface becomes ever more fragile and porous.
The tooth structure that lies underneath the lid (the most affected area) can experience mineral loss on the order of 30 to 50%.
▲ Section references – Dean, Fejerskov
White spot lesion vs. cavity – What’s the difference?
While a relatively arbitrary differentiation, as long as the surface lid of the affected area retains enough structural integrity that it remains intact (including when tested by your dentist with their tools), the lesion is still considered a white spot lesion.
If instead portions of the lid have broken down and have resulted in a substantial break in the continuity of the tooth’s surface or an outright hole, the lesion is then considered a cavity.
The importance of differentiating between these two states lies in what treatment options are considered possible and appropriate. (This entire subject is discussed in more detail below.)
d) How long does it take white spots (incipient lesions) to form?
The process of demineralization occurs anytime a tooth’s enamel surface is subjected to an acidic environment (like that which exists underneath a coating of dental plaque). But it takes a period of time before enough decalcification has occurred before it has affected the tooth’s enamel to the point where it is visible.
▲ Section references – Arruda, Harrell
e) Similar-looking lesions.
Another type of dental white spot is caused by an elevated systemic exposure to fluoride during childhood tooth development. This is an entirely different type of lesion than the one discussed on this page. It is referred to as fluorosis (use link for more details).
Differential diagnosis.
- White spots due to fluoride consumption will always have been present on the tooth from the day it first came in.
- In comparison, those related to cavity formation develop on areas of enamel that previously looked normal.
2) White spots and dental braces.
The formation of white-spot lesions can be especially disappointing for dental patients who wear conventional bracket-and-wire (fixed) orthodontic appliances. And if they form, they can ruin the expected perfect esthetics of having had braces.
a) The problem.
If not kept plaque-free, white spot lesions will tend to form around orthodontic brackets.
When the brackets are removed, the white spots will spoil the appearance of the teeth.
▲ Section references – Harrell
The added complication – Ruined esthetics.
With dental braces, there’s an added problematic twist. The tooth enamel that lies underneath the bracket will remain unchanged.
That means when the braces are finally taken off, the color difference between the damaged and undamaged areas may be very obvious (see pictures).
b) How quickly do they form?
While the time needed for formation will vary with the local conditions at each specific site, studies suggest that white spot lesions can form in as little as a month. (Arruda)
c) White spot / Dental braces incidence rates.
In separate papers, both Arruda and Dixon discussed studies that had evaluated the prevalence of white spot lesions among orthodontic patients.

White spot lesions resulting from poor home care during orthodontic treatment.
- On the whole, rates ranging from 2 to 96% were found to have been reported.
- A much-cited study from 1982 placed the rate at 50%, whereas more recent investigations (2009 and 2007) placed it in the 73 to 95% range.
- The patient’s teeth that are most affected are typically the upper front ones (15%).
- The teeth most commonly affected are the upper lateral incisors (23%). (The tooth with the largest white spot in our picture is a lateral.)
Then, in descending order, the canines (eyeteeth), 1st premolars, 2nd premolars, and then the central incisors. (Bourzgui)
▲ Section references – Arruda, Dixon, Bourzgui
3) How do you prevent white spots from forming?
a) Better brushing.
Since these discolorations are an early stage of cavity formation, the first line of defense in preventing them is to practice good oral hygiene.
Of course, doing so may be easier said than done, either from a standpoint of motivation or technical ability. (The use of an electric toothbrush may help some people with poor oral hygiene to improve their habits.) But bottom line, if no plaque is present, or else is removed in a timely fashion, no white spot lesions will form.
b) Using fluoride supplements.
Because the presence of fluoride in saliva assists the remineralization process (the action that helps to reverse the damage caused by tooth decay), making sure you have an appropriate exposure to it can help reduce your risk for these lesions.
Toothpaste, Oral Rinse
Using an over-the-counter fluoridated toothpaste (the best fluoridated toothpastes) or mouth rinse (like 0.05% sodium fluoride rinse) can be an effective way to get an adequate exposure. With higher-risk patients, the use of a (higher concentration) prescription product may be indicated.
Of course, patient compliance is an important factor. One study investigating this point found only 15% of orthodontic patients used their fluoride rinse daily as instructed. (Dixon)
▲ Section references – Dixon
Fluoride varnish.
A way of avoiding the need for patient compliance with those at high risk is the application of fluoride varnish. For example, some studies have evaluated its use with people who wear dental braces.
- One found a 7.4% incidence rate for white spot formation when the varnish was applied every 6 weeks vs. a 25.3% rate for the placebo group.
- Another study found a 44.3% reduction in lesions in a group receiving regular applications.
▲ Section references – Dixon
c) Using ACP/CPP-ACP products.
Calcium phosphate products (including amorphous calcium phosphate (ACP), casein phosphopeptide-ACP, calcium sodium phosphosilicate, and tricalcium phosphate) release both calcium and phosphate ions that may then aid with the remineralization process of tooth enamel.
▲ Section references – Arruda
Repairing white spot damage.
Generally speaking, anything that helps to promote tooth enamel remineralization will not only help to prevent white spots from forming but also, as discussed below, help to repair the damage that has caused them.
4) Evaluating and treating white-spot lesions.
White-spot lesions represent a very early stage of cavity formation, and possibly one where just a minimal amount of tooth damage has occurred.
- Only an examination by your dentist can lead to a decision that any specific white spot does or does not require treatment.
Ignoring what you see or making an uninformed decision on your own can result in significant tooth damage.
How your dentist evaluates white spot lesions.
1) Visualization of the lesion.
- Very slight (incipient) lesions may only be apparent after the tooth’s surface has been dried.
- More advanced lesions will be obvious white patches that show even when the tooth’s surface is wet.
2) Evaluating the integrity of the tooth’s surface.
Another gauge of the level of damage that has taken place that a dentist might use is to see if the tooth’s surface is still hard, smooth, and intact.
- To check, they may inspect the white spot with a pointed metal tool (a dental “explorer”). As they do, they will scrape and probe its surface to see if it’s still hard and smooth. (These are characteristics of healthy tooth enamel.)
- However, nowadays it’s realized that disrupting (destroying) the surface enamel of a white spot lesion by picking at it will interfere with whatever level of remineralization potential it may have had. And for that reason, this technique, if used at all, is practiced much less aggressively than it was historically.
3) Transillumination.
- They might place a strong light source on the backside of your tooth or else evaluate how the light from their overhead clinical lamp shines through.
- Deeper lesions (those having a greater degree of damage due to demineralization) will tend to block a greater amount of light as it passes through the tooth.
4) Inactive vs. active white spots.
Just as evaluating the amount of damage that has already occurred is vital, it’s also important for the dentist to judge the lesion’s level of current activity and potential to progress further.
- Active lesions tend to be located in areas of continued plaque accumulation, have a characteristic dull, chalky-white appearance, and evidence of surface breakdown (enamel roughness).
- Inactive or “arrested” white spots typically have a hard intact, shiny and smooth enamel surface. They may have a brown coloration (a result of picking up staining) and are found in areas where persistent plaque accumulation is not a problem.
5) Additional methods.
▲ Section references – Fejerskov, Dean
a) Truly incipient lesions will not require any treatment.
After their evaluation, your dentist may decide that at this point just minimal damage has occurred to your tooth and your lesion’s potential for further advancement is minimal.
If so, they may not recommend any formal repair but instead suggest that relying on the natural process of tooth remineralization is sufficient for arresting the disease process and restoring the damaged enamel’s strength and function.
If this solution is offered, the patient must understand that the healed lesion will forever remain as a chalky white patch on their tooth, although its surface should regain its lost shininess. In some cases, as remineralization occurs the affected area may pick up brown staining.
You’ll need to change your habits.
Keep in mind that this type of natural repair can only take place if you change the conditions that allowed the white spot to form initially.
Cavities are usually caused by some combination of ineffective brushing and flossing, and inappropriate sugar consumption. If you’re not able to change these conditions, remineralization cannot be expected to occur.
Helpful products.
As mentioned above, some types of compounds help to promote the remineralization process and their use can play an important role in tipping the conditions in a person’s mouth toward those of repair instead of continued destruction. This includes the use of fluoride and calcium phosphate products.
Monitoring will be required.
Since they represent an area that at least historically has been difficult for you to keep clean, any and all untreated white-spot lesions must be monitored by your dentist during regular checkups.
b) Treating minor unsightly lesions.
While some white spot lesions may not require outright repair, their appearance may be objectionable enough that some type of improvement is desired. If so, there are some relatively less-invasive remedies that might be attempted.
“Minimal” approaches for white spot repair –
1) Teeth whitening treatments.
It may be possible to use teeth-whitening treatments to mask the appearance of white spots. As the tooth’s color is lightened, its chalky-white lesion tends to become less noticeable.
The specific technique used might be a professional/in-office or at-home (strips, trays, paint-on) one. After the bleaching treatments have been completed, the patient can then decide if additional dental work is required to satisfy their esthetic expectations.
2) Resin infiltration technique.
One newer approach for treating white spots involves first etching the lesion’s surface with an acid conditioner and then bonding a flowable tooth-colored dental restorative into and over it.
▲ Section references – Dean
3) Enamel microabrasion.
A procedure termed “microabrasion” offers another possible remedy. This is a process where the surface of the tooth is worn and polished down using a hydrochloric acid and pumice mixture.
▲ Section references – Dixon
Less treatment may offer a better solution.
While none of the approaches above may give perfect results, if passable they can help to avoid the need for an outright repair (such as placing a filling or veneer), and the long-term maintenance required with it.
c) Some lesions will require repair.
If a white spot is unsightly or its surface has lost its integrity (it’s soft, rough, pitted or possibly has even developed a hole), some type of repair is indicated. If so:
- A filling is frequently used as a way of repairing or masking the damage. (Either dental amalgam or tooth bonding might be used, depending on the spot’s location.)
- With some front teeth, placing a porcelain veneer may provide the best solution toward fully restoring the tooth’s appearance and function.
Looking for more information?
If you’re having problems with white spots developing, this page will be helpful: Picking out a good anti-cavity toothpaste.
And, if you don’t really know how cavities develop, you might consider this page: How and why tooth decay forms. Knowing this info may help you prevent cavities in the future.
As an FYI read, you may find this page interesting: How dentists identify cavities on X-rays (with examples).
Last reviewed: April 25, 2026
Author: Paul Cotner, DMD — retired dentist.
Published by: WMDS, Inc. — owner of Animated-Teeth.com.
Educational information only — not a substitute for professional dental care.
Page references sources:
Arruda AO, et al. White-spot lesions in orthodontics: Incidence and prevention.
Bourzgui F. Orthodontics – Basic aspects and clinical considerations.
Dean JA, et al. McDonald and Avery’s Dentistry for the Child and Adolescent.
Dixon J. Prevalence of White Spot Lesions during Orthodontic Treatment.
Fejerskov O, et al. Dental Caries The Disease and Its Clinical Management.
Harrell RE. The relationship between appliance therapy and self-care.