Looking for information about other Dental Topics?
Full Website Index• Animated-Teeth.com •

What causes Canker Sores? (aphthous ulcers) – A list of outbreak triggers and risk factors.
What causes canker sore outbreaks?
If you suffer from aphthous ulcers—better known as canker sores—you may have noticed that certain experiences or exposures often seem to come just before an outbreak. If you’ve had that suspicion, you’re probably right.
Research shows that many different events, conditions, and substances can trigger canker sores. Still, the cause-and-effect relationship is difficult to pin down, since what sparks an outbreak in one person may have little or no effect on another.
This guide outlines the range of potential triggers and risk factors that have been suggested, helping you know what to watch for and hopefully experience fewer outbreaks.
Known and suspected canker sore causes and risk factors.
Here’s a list of possible outbreak triggers we discuss on this page.
- Trauma
- Tobacco Considerations
- Stress
- Nutritional Factors
- Foods
- Sodium lauryl sulfate (SLS)
- Hormonal Factors
- Genetic Factors
- Infectious Agents
- Medical Conditions
- Medications
Of course, YMMV.
As a prelude and a reminder, when reading through the outbreak factors discussed below it’s important to keep in mind that while many of them may be significant causes for some people, for others, including probably most people, they’re not factors at all.
So, if you find something on this page that doesn’t correspond with your experiences, it’s not that our information is inaccurate. It’s just that you’re one of the lucky ones, at least when it comes to that specific causative agent.
Note: Not all triggers are definitively proven.
And that’s precisely why we’ve used the words “known and suspected” outbreak triggers in this page’s title.
All of the causes we explain below are routinely included in scientific papers and textbooks that cover the subject of canker sores. And we would consider leaving any one of them out an omission. But it will take further research to confirm some of these causes definitively.
Here’s what’s so interesting about the subject of canker sore causes.
As you read through our information below, it should cross your mind that …
- The wide variety of outbreak triggers that exists suggests that a common disease process is involved …
- But the specific way it’s set off in different subgroups of people varies.
And that is exactly correct.
The science of the matter is that it’s the response of your own immune system that actually causes your aphthous ulcerations to form. It’s only the way that this response is triggered that varies between people.
Fundamentally, it’s the presence of antigens that’s the culprit.
In regard to your immune system’s response, it’s its detection of antigens (“foreign” molecules) in the oral tissue where your ulceration forms that sets the process of lesion formation into motion. So, in our discussion below, we try to explain how or why each factor facilitates/alters the antigen/skin tissue/immune system relationship.
▲ Section references – Neville
Known and suspected causes/triggers/predisposing factors for canker sores.
A) Mechanical trauma.
For many people, the formation of their aphthous ulcers is preceded by some type of tissue damage or trauma to the area where their lesions appear.
- This might be an accidental self-inflicted bite, irritation caused by the sharp edge of a tooth that needs repair, trauma from food (like a crisp chip), or even just overenthusiastic tooth brushing.
- A study by Casiglia reported that 38% of its subjects felt that their canker sores were initiated by some type of tissue trauma.
A biological explanation for this phenomenon.
▲ Section references – Casiglia, Chaven, Neville
B) Tobacco use / Smoking.
Researchers have noticed that when people initiate a habit of tobacco use (either smoking cigarettes, a pipe, etc… or the use of smokeless/chewing tobacco) their frequency of canker sore outbreaks tends to decline.
And if able to quit their habit, just the opposite occurs and their outbreak frequency is found to increase.
A biological explanation for this phenomenon.
The use of tobacco products irritates soft oral tissues. And in response, the surface of these tissues becomes more keratinized (their cells experience a build-up of keratin, a fibrous protein).
This keratinization effect serves to “toughen up” the skin’s surface, which makes it a more effective barrier to antigen entry. When tobacco use is ceased, the source of the irritation is removed and the skin’s surface reverts back to more normal (more penetrable) conditions.
An additional explanation.
Tobacco contains the compound nicotine. And when it’s present, it inhibits the release of Tumor Necrosis Factor-alpha (TNF-alpha) and other chemical mediators that play a role in a person’s immune system response that leads to canker sore formation.
▲ Section references – Chaven, Preeti
C) Psychological stress.
Many people find that their canker sores coincide with periods of emotional stress. Even the routine psychological fluctuations we experience on a daily basis in coping with minor events and changes can be enough to cause a person’s outbreaks.
As corroborating evidence for this observation, it’s reported that patients who have psychological disorders tend to have a higher incidence rate of experiencing aphthous ulcers. So do people who have genetic conditions that cause increased anxiety traits.
A biological explanation for this phenomenon.
It’s not so clear how this factor helps to trigger the immune system response that causes a person’s canker sores.
▲ Section references – Casiglia, Preeti
D) Dietary issues.
Canker sore outbreaks may be associated with nutritional deficiencies. Some of the vitamins and nutrients thought to be involved are:
- Vitamin deficiencies: B1 (thiamine deficiency), B2 (riboflavin deficiency), B6 (pyridoxine deficiency), B12 (pernicious anemia), C
- Nutrient deficiencies: zinc, folic acid, iron, selenium, calcium
A biological explanation for this phenomenon.
▲ Section references – Ship, Neville
E) Compounds in foods.
It’s very common for people to report that the consumption of various kinds of foods and beverages causes their canker sore outbreaks. Examples include:
- Cereal grains: buckwheat, wheat, oats, rye, barley, the gluten protein found in grains
- Fruits and vegetables: lemons, oranges, pineapples, apples, figs, tomatoes, strawberries, eggplant
- Dairy: cow’s milk, cheeses
- Other foods: nuts (walnuts), peanuts, almonds, chocolate, shellfish, soy, vinegar, French mustard, tea, coffee, cola
- Additives: cinnamaldehyde / cinnamon oil (a flavoring agent), benzoic acid (a preservative), dyes
- Other substances: toothpaste, mints, gums, dental materials, metals, medications
A biological explanation for this phenomenon.
It’s generally considered that chemical compounds found in these foods and beverages are themselves the triggering antigen for the immune system response that causes the person’s canker ulcerations.
Keeping a food diary.
▲ Section references – Woo, Neville
F) Sodium lauryl sulfate (SLS).
Some studies suggest that the use of oral care products that contain sodium lauryl sulfate (“SLS”), a foaming agent found in most toothpaste and mouthwash formulations, may place a person at increased risk for canker sore breakouts.
Research findings.
- Several early studies reported that test subjects who used SLS-free toothpaste experienced fewer canker sores. One study found this reduction to be as high as 81%. (Chahine)
This same study also stated that some subjects reported that their aphthous lesions that did form were less painful than the ones experienced during periods when they continued to use products that contained SLS.
- It should be noted that other studies have not been able to replicate all of these same findings.
For example, a more recent study by Shim found that while the use of an SLS-free toothpaste did reduce ulcer duration and pain levels, its use did not help to reduce the overall number of outbreaks that the test subjects experienced.
A biological explanation for this phenomenon.
We’ve seen two mechanisms given as an explanation for this effect.
SLS affects skin tissue surfaces.
Some papers suggest that SLS has a denaturing (molecular altering) effect on oral tissues. As a result, the skin’s surface provides a less effective barrier to antigen entry.
The other proposed explanation is that the SLS molecule itself is the triggering antigen.
▲ Section references – Chahine, Shim, Neville
G) Hormonal changes.
For women, there may be a relationship between aphthous ulcer formation and certain phases of their menstrual period. It’s also been reported that some women notice fewer sores during pregnancy. Neither of these observations has yet been adequately documented or explained by research.
A biological explanation for this phenomenon.
▲ Section references – Neville
H) Genetic factors.
Data suggests that some people may have a genetic predisposition for experiencing canker sores.
- It’s been reported that 35% of people who get lesions have at least one parent who suffers from them too.
If both parents experience them, there’s a 90% chance that their child will too.
- In the case of identical twins, if one suffers there’s a 91% chance that the sibling will too. The correlation with fraternal twins is only 57%.
- Those people who have a positive family history typically get their first ulcers at an earlier age and experience more intense symptoms.
A biological explanation for this phenomenon.
▲ Section references – Casiglia, Akintoye, Slebioda
I) Infectious agents –
Bacterial.
The current thought is that bacteria are not a causative agent for canker sores but instead, it’s some chemical compound associated with their presence and/or the infections they cause.
- One research study found 95 different bacterial species associated with their test group’s canker ulcerations. Only 3 of these species were found in the mouths of the control group. (Casiglia)
This correlation suggests that their presence may be related to canker sore formation.
- Some studies have suggested a relationship between Streptococcus sanguis (a type of bacteria that can cause tissue damage) and the formation of canker sores. However, this theory is still unproven. (Chavan)
Viral.
Some viruses may cause aphthous ulcer formation.
Some of those suspected are: cytomegalovirus (CMV), human papilloma virus (HPV), human herpes virus-8 (HHV-8), Epstein-Barr virus (EBV), human immunodeficiency virus (HIV), and Varicella zoster.
A biological explanation for this phenomenon.
▲ Section references – Casiglia, Chavan, Neville
J) Medical conditions.
Several medical conditions have been reported to show a correlation with canker sore formation (and other forms of aphthous ulcers as well). This finding suggests that people who experience persistent difficulties with mouth ulcers should consider the possibility that an underlying undiagnosed systemic condition exists.
Some associated medical conditions are: Behcet’s disease, neutrophil dysfunction diseases, inflammatory bowel diseases (celiac, Crohn’s, ulcerative colitis), HIV-AIDS, MAGIC syndrome, Reiter’s syndrome, systemic lupus erythematosus, cyclic neutropenia, Marshal’s syndrome, and Sweet’s syndrome.
A biological explanation for this phenomenon.
▲ Section references – Neville, Chavan, Ship
K) Medications.
The use of nonsteroidal anti-inflammatory medications (NSAIDs), beta-blockers, chemotherapeutic agents, and the compound nicorandil have all been suggested as being risk factors for canker sore outbreaks.
A biological explanation for this phenomenon.
▲ Section references – Neville
L) Are they contagious?
No, canker sores are neither contagious nor infectious. We explain why on this page: Why aphthous ulcers are not contagious.
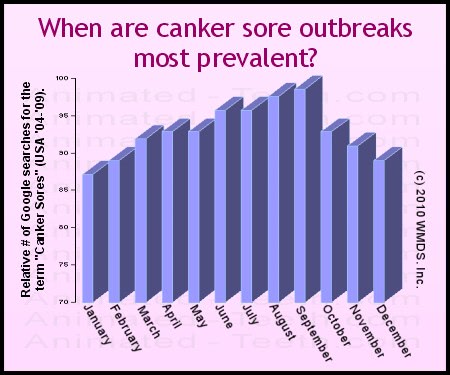
When do most outbreaks occur?
There may be a seasonal tendency for canker sore outbreaks. If there is, it seems that people tend to suffer from them more during the summer months.
Our “research.”
What we did was evaluate Google search volume for the keywords “canker sores” over a 5-year period.
The chart we created from that data shows that web searches tend to rise into and subsequently top out during the summer months (August into September). They then fall off, reaching a low point in December and into January.
As you can see below, a similar analysis involving the term “mouth ulcers” seems to show the same seasonal bias.
(Aphthous ulcers are the most common type of recurring mouth ulcer. And for those who initially don’t know what type of lesion they do have, the generic term “mouth ulcers” seems a logical choice to use for an initial search.)
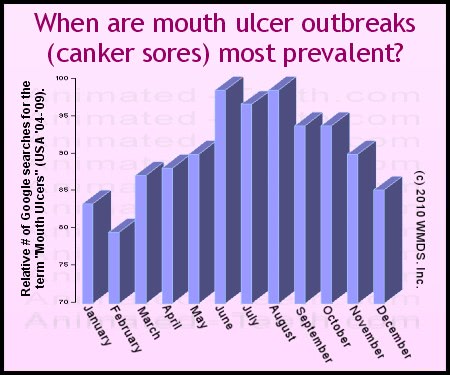
We aren’t trying to pass our simple study off as hard and proven facts. But what it shows is interesting.
Our hypothesis.
In regard to an explanation, one risk factor for outbreaks is allergies to food, including fruits and vegetables. The increased availability of these items during the summer months might explain the seasonal effect demonstrated above.
Last reviewed: August 19, 2025
Author: Paul Cotner, DMD — retired dentist.
Published by: WMDS, Inc. — owner of Animated-Teeth.com.
Educational information only — not a substitute for professional dental care.
Page references sources:
Akintoye SO, et al. Recurrent aphthous stomatitis.
Casiglia J. Recurrent aphthous stomatitis: Etiology, diagnosis, and treatment.
Chahine L, et al. The Effect of Sodium Lauryl Sulfate on Recurrent Aphthous Ulcers.
Chavan M, et al. Recurrent aphthous stomatitis: a review.
Neville BW, et al. Oral and Maxillofacial Pathology. Chapter: Allergies and Immunologic Diseases.
Preeti L, et al. Recurrent aphthous stomatitis.
Slebioda Z, et al. Recurrent aphthous stomatitis: genetic aspects of etiology.
Shim YJ, et al. Effect of sodium lauryl sulfate on recurrent aphthous stomatitis: a randomized controlled clinical trial.
Ship J, et al. Recurrent Aphthous Stomatitis.
Woo S, et al. Recurrent Aphthous Ulcers: A Review of Diagnosis and Treatment.